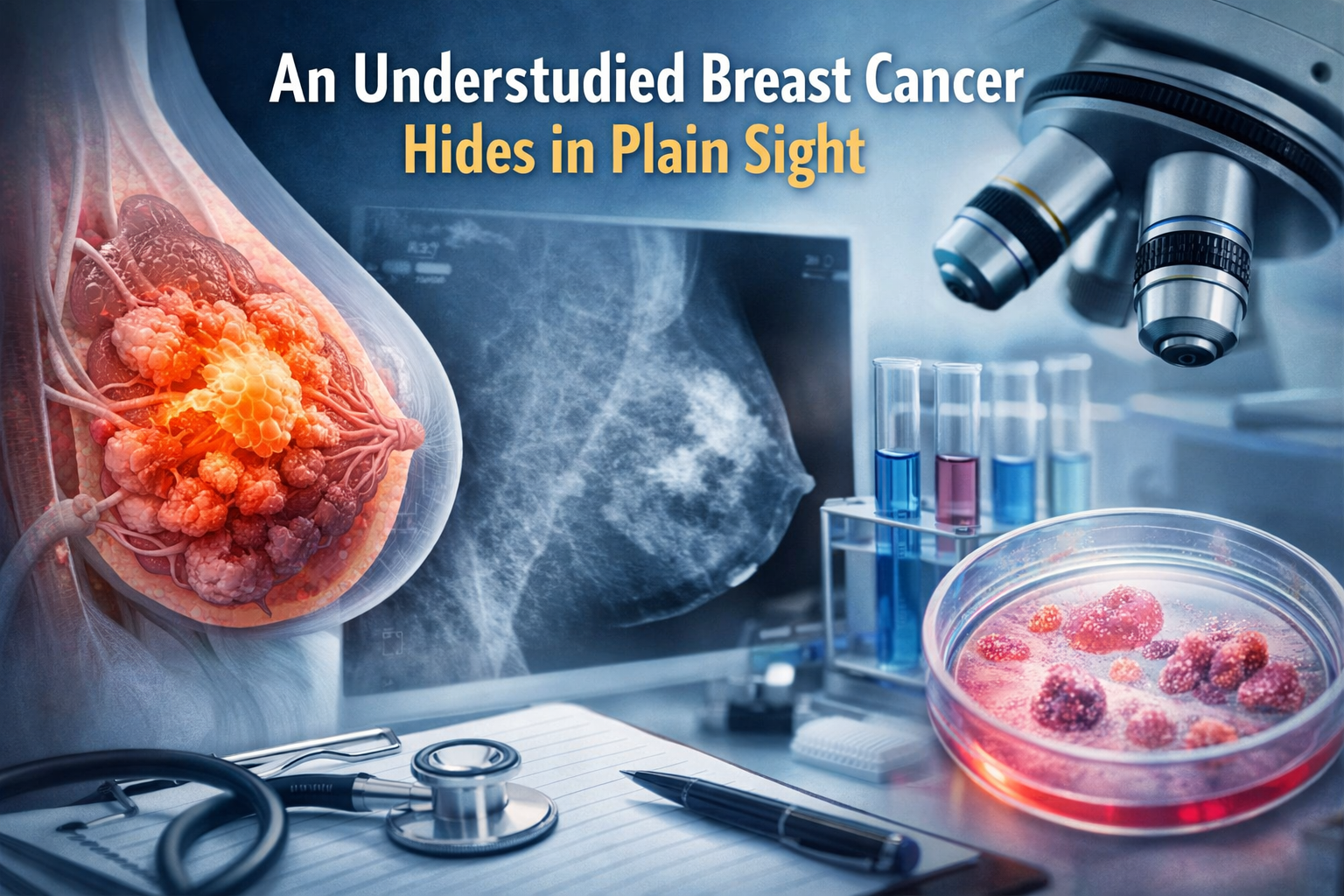
Invasive lobular carcinoma, or ILC, is the second most common form of breast cancer, accounting for about 10 to 15 percent of cases. Despite its prevalence, it remains less studied than invasive ductal carcinoma, which continues to dominate breast cancer research and clinical trials.
ILC grows differently from other breast cancers. Instead of forming a firm, easily detectable lump, the cancer cells spread in thin lines throughout the breast tissue. This diffuse pattern makes the disease harder to detect using standard imaging techniques like mammograms and ultrasounds. Many patients are diagnosed only after tumors have grown large or spread beyond the breast.
The biology of invasive lobular cancer is also distinct. Most ILC tumors are estrogen receptor positive and HER2 negative. Many show loss of the CDH1 gene, which affects cell adhesion. Without this gene, cancer cells separate easily and migrate in ways that are more difficult to track and treat.
Treatment options for ILC are often based on studies of invasive ductal carcinoma. Very few clinical trials focus on lobular disease. This leaves doctors with limited evidence to guide decisions about surgery, systemic therapy, and long-term management.
ILC also spreads differently from other breast cancers. Metastases are more likely to appear in the gastrointestinal tract, ovaries, uterus, and peritoneum. These areas are not always included in routine surveillance, which can delay detection of recurrent disease.
The cancer is more common in postmenopausal women and has been associated with hormone replacement therapy. Another challenge is its tendency to recur late. Some patients experience relapse 10 or more years after their initial diagnosis, long after routine follow-up ends.
Funding matters now. Targeted research funding could significantly improve outcomes for invasive lobular cancer. It would directly support the development of imaging techniques that are better suited to detecting diffuse tumors. Furthermore, funding would stimulate clinical trials specifically focused on ILC to refine surgical, hormonal, and systemic therapies. Grants would facilitate research into the metastatic patterns unique to ILC and encourage the discovery of biomarkers for earlier detection and more personalized treatment. Increased funding would provide the resources needed to explore areas of ILC biology that have remained unexplored for decades.
Cancer research funding decisions determine which patients benefit from advances and which are left behind. Patients with invasive lobular cancer have waited too long for studies that reflect the true nature of their disease. Investing in ILC research is essential for developing more precise treatments and improving outcomes for tens of thousands of patients each year. As funding priorities are debated and budgets reviewed, invasive lobular cancer should no longer be overlooked.